Abstract
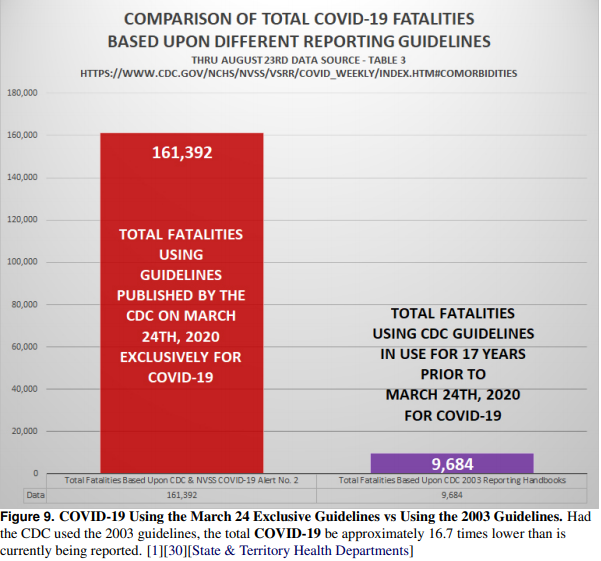
According to the Centers for Disease Control and Prevention (CDC) on August 23, 2020,
“For 6% of the deaths, COVID-19 was the only cause mentioned. For deaths with conditions
or causes in addition to COVID-19 , on average, there were 2.6 additional conditions or
causes per death.”[1] For a nation tormented by restrictive public health policies mandated for
healthy individuals and small businesses, this is the most important statistical revelation of
this crisis. This revelation significantly impacts the published fatalities count due to COVID-19.
More importantly, it exposes major problems with the process by which the CDC was able
to generate inaccurate data during a crisis. The CDC has advocated for social isolation,
social distancing, and personal protective equipment use as primary mitigation strategies in
response to the COVID-19 crisis, while simultaneously refusing to acknowledge the promise
of inexpensive pharmaceutical and natural treatments. These mitigation strategies were
promoted largely in response to projection model fatality forecasts that have proven to be
substantially inaccurate. Further investigation into the legality of the methods used to create
these strategies raised additional concerns and questions. Why would the CDC decide
against using a system of data collection & reporting they authored, and which has been
in use nationwide for 17 years without incident, in favor of an untested & unproven system
exclusively for COVID-19 without discussion and peer-review? Did the CDC’s decision to
abandon a known and proven effective system also breach several federal laws that ensure
data accuracy and integrity? Did the CDC knowingly alter rules for reporting cause of death in
the presence of comorbidity exclusively for COVID-19? If so, why?
Conclusions
Arguing over what the most accurate COVID fatality count may be is an exercise in futility without
intimate knowledge of case history and accompanying certificates of death, and it is the exact reason
we entrust these determinations to the skill of our licensed professionals.With the inclusion of probable fatalities and significant changes made to how
certificates of death are recorded exclusively for
COVID-19 , scientific objectivity demands that we
acknowledge the data presented is inaccurate.
Federal agencies have a legal obligation to
provide the most accurate data to the public, fellow agencies, and policy makers they are advising, and they have a responsibility to abide by
every federal law. This responsibility to collect,
analyze, and publish data accurately, transparently,
and with unquestionable integrity increases exponentially during a national crisis.
It is concerning that the CDC may have willfully
failed to collect, analyze, and publish accurate data
used by elected officials to develop public health
policy for a nation in crisis.
Further federal investigation is justified by the
magnitude of the crisis and the collateral damage
generated by policies based upon projection data
that was unproven and never peer reviewed. If the
data being reported was indeed compromised by
the CDC’s perplexing decision to abandon proven
data collection and reporting practices in favor of
untested methods, then all public health policies
based upon these inaccurate data must be reexamined